 |
A Lewinian Taxonomy of Psychiatric Disorders
by Matthew Maibaum (Fonte)
Kurt LEWIN wrote briefly, but with considerable depth, about his conjectural ideas about mental disorder, termed ”Unreality”, and primarily from a developmental point of view. This paper, based upon this author‘s studies of LEWIN and his theorizing about the growth of levels of reality, and boundaries, will discuss some theorized bases of major mental disturbances as they would be explained, and explainable, according to Lewinian field theory. To some degree comparison will be made with other major theories about the development of these disorders. A topological psychology perspective of the major features of select mental disorders from DSM IIIR will be presented, and with this the postulated central features of those disorders according to a Lewinian analysis. Some special attention will be paid to disorders that have been elusive to both etiology explanation, and cure, in traditional viewpoints in psychiatry and clinical psychology. By way of conclusion it will be suggested that, and where, classical Lewinian field theory may have a whole other analysis available to the study of mental disorders and to some specific conditions that have been elusive according to other, historically ”clinical” theories. Printed and projected pictures of Lewinian figures will accompany the talk if/where possible).
We have elaborated ways in which a Lewinian topological system of thought can be concurred with other ways of viewing pathological process, particularly utilizing the ways those processes are seen by psychoanalytic thinking, and to a lesser degree utilizing the ways those processes are seen in behavioral psychology thinking.[1]
It may not be beyond reason to go further than to illustrate clinical syndromes in a new way, using what has been basically a theoretical explanatory system from social psychology, and to then try and use the kinds of insights that using that system can suggest, to construct insights into the very etiology of mental disturbances. If this social psychological model of viewing behavior and mental process can illustrate areas of pathology that have been the province almost entirely of other types of theories, one can try and move from the descriptive to the explanatory in the use of that model. It is true that view will explain processes it is used to look at in ”its own terms”, not more familiar ones. But such attempt can be made.Where new tools are used, new things may be turned up; it is not only true necessarily that old things will be seen, and left still unexplained any better, in a new light.[2]
Psychological theory, particularly psychoanalytic theory, has talked about the developmental importance of sense of ”boundary” between self and the outside world. Developmental psychoanalytic thinkers have described the growth of ”ego boundaries” in the child to adolescene as a concomitant in development and an essential element in the definition of the ”self” apart from the environment and apart from the mother. Ego boundaries comprise in part, as psychoanalytic thinkers define them, the boundary conceived by the child to exist between what goes on in the ”self”, and outside the self in the immediate (and farther) environment. The formulation has not been dealt with much, if at all, in topological psychology and topological psychology has not been utilized to describe these psychoanalytic developmental psychology formulation.
It would appear that a very simple representation of the growth of the ego boundary would involve the conceptualization of a boundary forming between the self, and the surrounding lifespace as such: simply, in Lewinian terms, the boundary around the ”P”, Person, separating him from his life space.
Crucially however another thing must happen. And that is, the child must learn moreover at some point early in his life another sort of boundary only somewhat less crucial to him. It is the boundary between that realm of his environment in which ”facts” occur that are of importance and relation to him, and that realm of his environment where things do not concern him to the point of emotional and physical reaction that would be appropriate. This can be conceived of in Lewinian terms as a boundary too. In topological representation, it would be placed not between the Self, the Person, and the life space, but between the inner area of the life-space, and the outer area of the life-space. Were the life space of a person to be conceived of as a sort of representation of Saturn and all her rings, concentric to one another, this boundary between the ”relevant” and the ”nonrelevant facts” of the person´s life space could be conceived of as the ring at median distance out from the planet, so to speak. For want of a better term, this boundary within the life space could be termed not an ”ego boundary” but a ”relevance-boundary”. And as said, in some individuals this boundary develops poorly. Some individuals cannot distinguish between things in their environment they should react to, and things that should not. In some others, that boundary forms strongly as they develop, but too close in. They do not react with responsibility and emotional depth to things that they should, hence the classic schizoid as he is contemporarily defined and described. In others it develops but too far out: and they react with too much responsivity and emotionalism to things that do not bear them relevance meriting that, and usually in a negative way. They feel threatened by things they need not feel threatened by. Hence the paranoid disorders´ perhaps most noticeable feature. (See Figure 3-1).
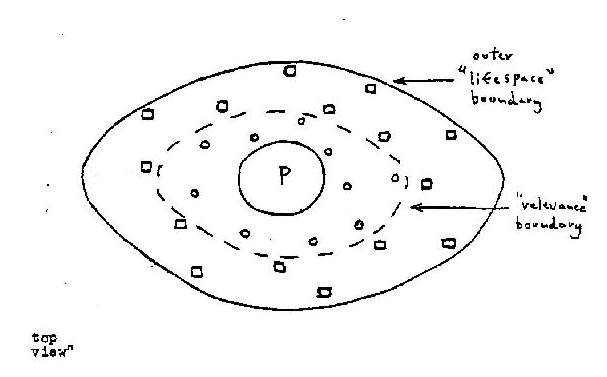
Figure 3-1:The "Relevance Boundary" In the Life Space (Postulated) / Circles -> "facts" important to relate to Squares -> "facts" not important to relate to
Psychic mechanics of the foundation of the ego boundary, and why it forms where it does, has never been completely explained by psychoanalytic thinkers. And it would be best to leave discussion of those aspects of the boundary formation process to them. However, a topological analysis of what the process looks like, with clinical features, leads one to suggest that both schizoid and paranoid disorders stem primarily from a developmental deficit in the placement, and strength, of the psychological boundary that leads an individual to decide what is relevant to react to, and what is not.
There would appear to be another kind of problem found across the clinical syndromes we observe, when we look at them in terms of topological psychology. It seems to be a problem an individual has wherein his self, innermost psychic processes in the self, perceive facts in the environment in a more intense way, or in a less intense way, than most other people in his circumstances would. This level of emotional reactivity and perceptual detail could be termed, in topological psychology, ”vector intensity”. From a clinical point of view, the ”vector intensity” of facts in the life space of the manic patient for example is heightened pathologically, hence his manic reactivity and emotionalism when interacting with anything but the simplest, and most pacifying of environments and even, sometimes, them. And the vector intensity of the severely depressed patient is drastically lowered. He reacts in a lowered emotional way, and even his perceptions seem dulled, limited, with respect to facts in his life space. In severe depression as we know, facts that appear to others around him are treated by him as if they do not exist. The common feature across both problems of ”vector intensity” is that for whatever reason, the perception of facts by the psyche of the self and/or the reaction to these is either diminished or elevated, as if the energy available to the self/psyche for relating to facts in the life space is either too much, or to little. That energy level disorder probably relates mostly to the mechanics within the psyche itself, mechanics the details of which are outside the central area of interest of topological psychology at this time. (See Table 3-1; all tables in 2nd part).
Movement of the self´s energies towards ”facts” includes efforts to perceive events, efforts to react to events, efforts to incorporate new facts or events into the life space in some circumstances, and efforts to either delete events and facts from the life space or deny their existence (as in pathological processes may be the case). Problems in the use of energies by the Person/Self in efforts to relate to facts, may be termed ”processing disorders” in that they involve problems of the self´s processing information about facts in the life space, and problems in relating to facts in the life space. (See Table 3-1).
A problem in this realm could balled for want of a better term, ”processing efficiency”. The effort made by the psyche to perceive facts and their details, and to react to facts in the life space, is muddied up in some kind of way such that either the facts are not perceived as they are, or they are not related to in such a way by the psyche and upon the motivation of the psyche such that the needs of the person are adaptively met, or both. The datails of facts are not perceived too intensely, or too weakly, as in vector intensity disorders. Rather the holistic efficiency of processing aspects of ”facts” is poor, or the response mounted to facts by the psyche (e.g., behavior) is missing some important elements, such that an effective interaction with facts in the environment is not made. One kind of problem, and the chief one found in many schiziphrenias, but not the only kind of problem, could be called distortion. Because some aspects of facts are interpreted and responded, and other features of facts are not, the facts are perceived by the psyche/self as differently in quality than they really are and are related to in a maladaptive way by the person. (See Figure 3-2, Table 3-2).
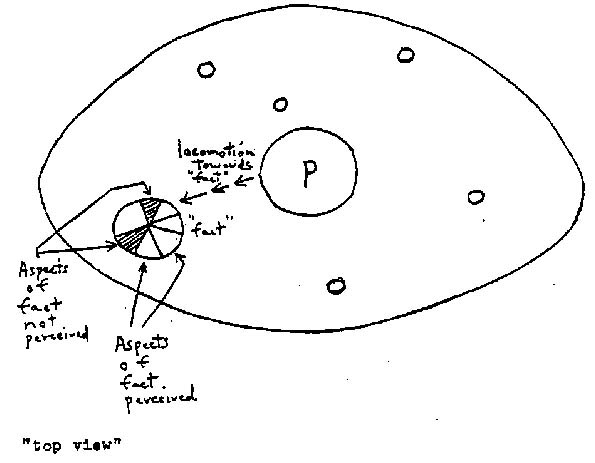
Figure 3-2: Processing Deficits as Sometimes Realised in Dementias and Other Syndromes
A very broad theoretical relationship between some types of disorder and the quality of perceptual process, and vector intensity, is presented in Table 3-3.
A very broad theoretical relationship between some disorders, and level of processing efficiency, vector intensity, level, and placement position of the person´s ”relevance boundary” altogether, is expressed in Table 3-4.
It is suggested that problems in a person´s self/psyche´s ”vector intensity” vis a vis a wide variety of ”boundary deficit” problems provide the primary arena of problem in manic-depressive disorders. It is suggested that in bipolar disorders of the cyclothymic type, and moreover in manic-depressive disorders of the cyclical type, some disorder in the availability of perceptual and reactive energies within the self/psyche itself available for relating to facts, is the root of vector intensity problems.
It is suggested that in topological terms, problems in ”processing efficiency” that have their root in the use of energies for perception, encoding of information, and reaction to facts of the environment, within the self/psyche, are the core of the problems found in the schizophrenic disorders, and in organic brain syndromes, and that anxiety attendance is a secondary feature to these.
These concepts will be discussed in more detail in following sections.
Some attention should be paid to processing deficits. It is theorized that there are important relationship between the energies expended by the self/psyche towards facts, and the ”qualities” of facts that are there to be perceived and interpreted and responded to by the person.
One proposes readily that there are subsidiary aspects to any fact. A ”fact” is composed of aspects that distinguish it from another fact, and that indeed lead the self/psyche to decide upon perceiving it and attending to it and indeed how to relate to it. The encoding by the self/psyche upon expending its energies, of information about specific facts such that it then leads the person to respond as he does to each fact, can be termed here ”content information coding”.
But there is another aspects to the encoding process of aspects of the facts. From a sheer physical, perceptual view facts may be composed of ”composite” aspects, sub-features. But from a clinical point of view we are told that what LEWIN called a ”fact”, what Freudian psychology to all intents and purposes here termed an ”object”, has qualities that elicit emotional responses in the self/psyche of the perceiving person. The emotional qualities of a fact and its component aspects are the aspects of it that lead the person to the type of response that he will make to it. And the encoding of these aspects of a fact can be termed ”emotional quality encoding”.
It is theorized here that the self/psyche of the person can have deficits in two types of process, two types of processing deficits thus. One is in content information encoding itself, the other in emotional quality encoding. In the latter, in some way emotional qualities attendant upon specific aspects of a fact, are not emergent in the self/psyche of the individual. He does not perceive aspects in facts and then have an emotional quality encoded with that aspect of the fact, at the same time. It is further theorized that where the person does not perceive content information, or emotional quality elicitors in a ”fact”, he will not respond reciprocally in an appropriate way to the fact and to its fuller aspects, and his behavior will then either be unsatisfying, or inappropriate.
This above theory has little direct relevance to topological psychology as classicly defined and has more relationship to ”communication-information” theories, to cognitivist psychology, and to some degree to perceptual psychology as applied to clinical situations. But when a processing deficit type of analysis as above is combined with an analysis of ”boundary deficit problems” this bears more relevance to the uses of topological psychology in defining aspects of abnormal problems.
One can theoretically postulate four conditions looking just for the moment, at major types of processing deficit, combined with major problems of ”boundary disorder”. One can postulate that an individual can in the processing deficit dimension, or realm, have deficits mainly in ”content information coding” relative to facts in his life space or problems in ”emotional quality encoding” relative to facts in his life space. These deficits can stem from internal mechanism deficits in his self/psyche or in the way he ”locomotes” towards in Lewinian terms, i.e., perceives and approaches, facts in his life space.
In a second dimension he can have problems in ”boundary placement”, problems in the location appropriately of his ”reference boundary” for the most part and, in a few disorders, theoretically, problems in the location of the outer boundary of his life space. His reference boundary can be located in his life space through development processes, too distal, too far out so to speak from the self/psyche, or too basally, too close in so to speak, to the self/psyche. It is theorized that in individuals where there is a significant processing deficit in the content information coding realm, and where the reference boundary is located too distally, an ideal combination of factors is created for the paranoid personality, and to some degree for other paranoid phenomena such as the emergence of paranoid states, and paranoid schizophrenia. Where there is a processing deficit in content information coding and the reference boundary is too basally located, an ideal combination of factors would appear to be present for creating a schizoid personality. It is theorized that where the processing deficit exists and is severe in the emotional quality coding area, and the referent boundary of the person is too distally located, an ideal situation is present for the creation of a passive-dependent personality that becomes hysterical under stress, particularly where too many ”facts” that should not be dealt with in the life space are invested with emotional meaning and are reacted to by person´s self/psyche, and where emotional quality aspects of facts heavily outweigh in perception, content information aspects of those same facts.
Lastly it is suggested that where there are important processing deficits in emotional quality coding, and the referent boundary is located too basally vis a vis the person´s life space, an ideal set of factors is created for the development and growth of a narcissistic personality with schizoid defenses. In this latter case this would be predicated particularly where the emotional qualitiy aspects of facts heavily outweigh the content information aspects of the same facts, and the self/psyche of the person reacts to only a few facts ”close to itself” and not to other facts of importance that it should. Those would include, importantly, emotional and physical responsibilities to others. (See Table 3-5).
Lastly we come to one final theoretical area of conjecture for the purposes of this study. That concerns the relationship of a fifth class of factor to topological psychology analyses of mental disorders, and to the other types of factors mentioned already. That factor is what can be called ”perceived stress”, stress as experienced by the person, and by his self/psyche, and the way in which it modifies perception and responsive behavior. From the standpoint of what topological psychology has to say, one can theorize about the character of some mental conditions based upon the way a high level of stress interacts with ”boundary disorders” to produce different types of mental disorder. (See Table 3-6).
Theoretically one can posit that there are two major classes of reaction by the self/psyche to perceived stress, at any age and across any age range. One is where as a result of reaction to stress, the self/psyche mounts a much stronger boundary as it were, between the self and the life space´s facts and events, as a simplistic defense over being overwhelmed by stimuli. The second is where the self/psyche does not mount an adequate degree of ”boundary” between the self, and the life space´s events and facts going on around the individual and, as it were, outside his head. Disorders of the first group all have in common the fact that the self/psyche mounts too strong a boundary between the self/psyche and the life space. As a result, accurate perception of facts in the life space is not possible and adaptive interaction with facts and events in the life space is not possible. One can term disorders found here, ”hypoecoic” process disorders. The second class of mental problems is to be distinguished by having in common the fact that an inadequate strength and degree of boundary exists between the mechanisms of the self and psyche, and the life space. From a Lewinian point of view, there is in common too much uncontrolled, randomized, unorganized, interaction between facts and events in the life space, and the perceptive, processing and reactive mechanism of the self/psyche. Problems of this type may be termed ”hyperesoic” process disorders. (See Table 3-7).
In disorders of the first group, given some level of stress and the fact that the organism cannot handle it, and given too much of a boundary between the self/psyche and the environment, the intensity of disorder will be a reflection of the strength and impermeability of the self/environment boundary combined with the level of perceived stress. Where the boundary, given a high level of perceived stress, is strong but not abnormally impermeable, the person seems somewhat ”normal”. Where the boundary is more inflexible and impermeable, and self/life-space interaction is more distorted, you see the clinical features common to the ”schizoid” individual, the isolar individual; the person with some autistic social and intellectual traits. Where the boundary is much more impermeable still, you find the severe clinical traits of autism. Leading symptomatic concomitants of each of these three general levels of degree of disorder are as follows. In the area between ”absolute normalcy” and isolar thinking, schizoid thinking and behavior, you find often massive anxiety at times, as a signal to the individual as an inability to asume challenges, alternating with long periods of seeming nonreactivity emotionally and socially to others. In the center of the schizoid realm you find these symptoms, and a lack of motivation and energy for emotional interaction with one´s surroundings moreover, as a massive defense in the individual against the additional stresses to be experienced through a competition of fantasies and thoughts in the person´s self/psyche with realistic requirements for his psyche to interact with the external environmental world. In the autistic range, you find a regression totally of the self/psyche in the absence of interaction with the environment, to fantastic, magical and fantasmic thinking within the self and a retreat to a level of primary physical functioning that has little reactive relationship to the surroundings, to things in the life-space. These are all well-know clinical signs of such disorders and these are those features that have greatest significance from the standpoint of topological psychology theory. (See Table 3-7).
In the hyperecoic disorders (Table 3-8) the boundary between self/psyche and life-space and events is inadequate. In these one can likewise postulate a progression as a function of weaknesses of that boundary, given an unmanageable high level of stress, progressively from normal, to neurotic, to schizotypal, to borderline schizophrenic to schizophrenic disorders. They can be conceived, from the standpoint of topological psychology, to not just be different disorders but to fit on a progression, as a function of a level of stress and as a function of a successively less effective self/environment boundary. Each disorder has key clinical concomitants of note to topological psychology. In the normal to neurotic range, where the individual has problems, one finds massive anxiety as a signal of danger. In the schizotypal range, one finds a retreat into wishful, hopeful, magical, and other irrational thinking, and avoidance of responsibilities, as a massive defense (with some commonalities to autistic thinking, likewise regressive) against emotional frustration and terror at problems provided by stresses from the outside environment. In the borderline schizophrenie and borderline personality types (as defined in DSM-III) one finds a massive destabilization of function that is usualy periodic, often with periods of psychotic symptoms that mimic a number of definitively described separate mental disorders. Here the individual´s self/psyche cannot manage interactions with the environment well at all and is, as it were, ”hanging on” and showing ”spot shortages” of capacity to function socially, interpersonally, and intellectually and emotionally in a variety of ways, often in sequence. In schizophrenia of the full-blown variety the person demonstrates any of a number of massive deficits in mental organization in the face of stress. In some subcategories, such as undifferentiated schizophrenia even of the residual type, where full-blown psychotic symptoms are not seen all the time, the individual demonstrates a seeming low energy and low motivation level to function as if his self/psyche has given up trying to relate to a life-space experienced to be too full of facts, and events, to manage or to relate to. The most compelling subtype of schizophrenia from the standpoint of topological psychology might be obviously the catatonic type, and there in the subdued rather than the excited subtype. According to historic clinical theory, the catatonic for whatever reason is inhibited from functioning rationally and adequately with his environment because his self/psyche experiences itself to be so overhelmed by the stimuli in the environment (the presence of facts and events) that it cannot interact with them in a way that is organized, discriminating, goal-effective and reasonably free of feeling overloaded. The behavior of the catatonics is either periodic pointless excitability, as in the excited type, or waxy flexibility and immobility as in the more common subdued type, perhaps the most well-know feature of the class. (See Table 3-8).
[1] Maibaum, Matthew, A Topological Approach to Abnormal Syndromes. Paper presented at second annual conference, Society for the Advancement of Field Theory, East Hanover, New Jersey, August 1988.
[2] The general overview of Lewinian psychology posited in this paper may be found in it´s original form in LEWIN, K., Principles of Topological Psychology, (New York: McGraw-Hill, 1936); and in LEWIN, K., Field Theory in Social Science (Dorwin Cartwright, Ed.), (New York: Harper Brothers, 1951).